When the damage to your shoulder joint is complex, particularly involving irreparable damage to the rotator cuff tendons, your surgeon may discuss a specialized procedure known as reverse shoulder replacement surgery. This innovative approach to joint reconstruction offers a possible solution for individuals who might not be candidates for a traditional shoulder replacement. In this post, we’ll cover what this surgery entails, when it is performed, and what to expect during the recovery process.
Key Takeaways
- Unlike a conventional shoulder replacement, this procedure reverses the natural ball-and-socket anatomy of the shoulder, placing the “ball” component on the shoulder blade and the “socket” on the upper arm bone.
- This anatomical reversal allows the large deltoid muscle to take over the primary function of lifting and moving the arm, compensating for the damaged rotator cuff.
- The most common reasons for recommending this surgery include cuff tear arthropathy (arthritis combined with a massive, irreparable rotator cuff tear) and complex shoulder fractures.
- The primary goals of the procedure are to provide relief from chronic pain and to restore a functional range of motion.
The Anatomy of a Healthy Shoulder
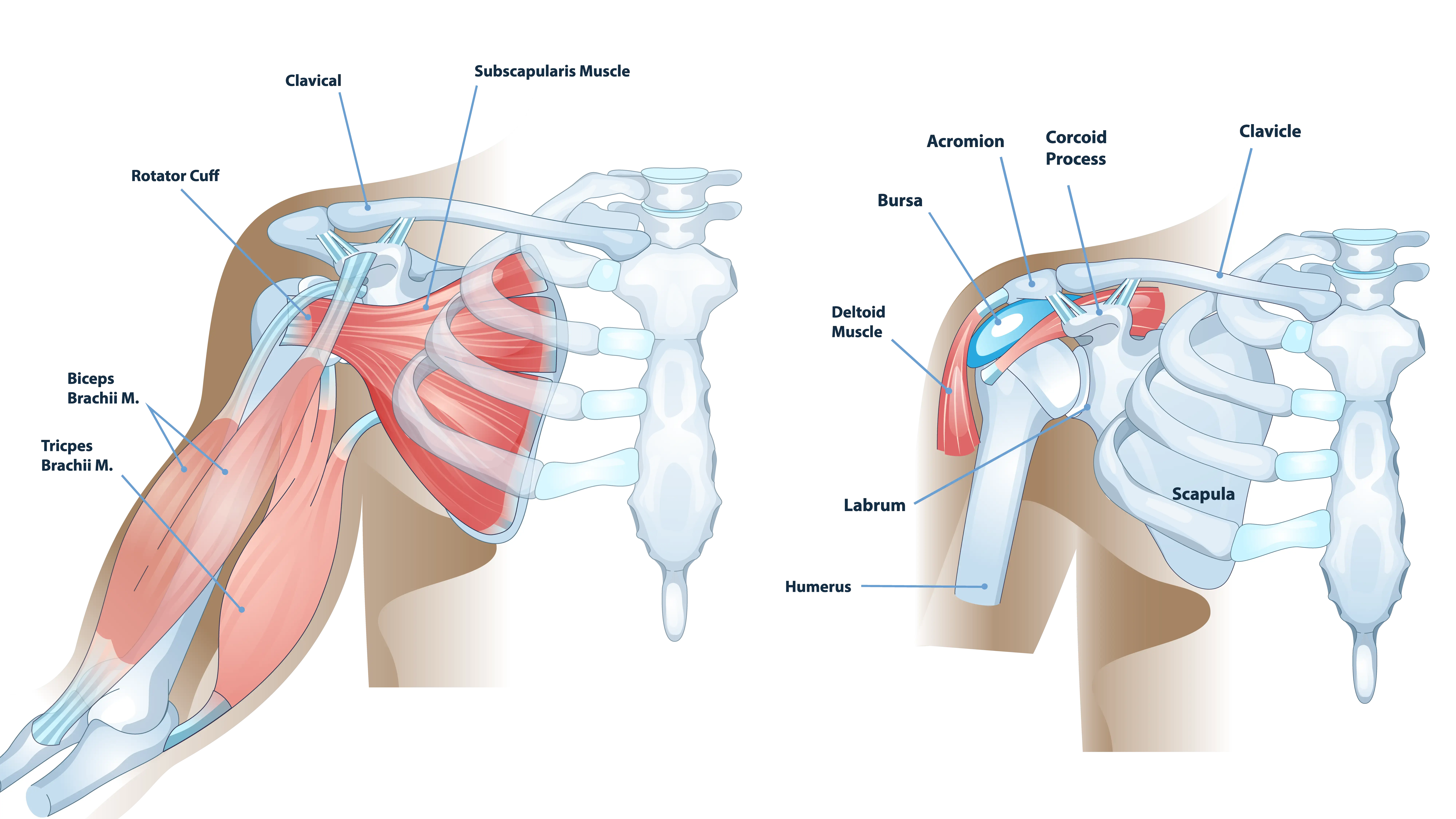
The shoulder is a ball-and-socket joint that provides the widest range of motion of any joint in the human body. The “ball” is the head of the humerus, the long bone of the upper arm, and the “socket” is the glenoid, a shallow cup on the shoulder blade (scapula).
This joint’s stability and movement are primarily controlled by two major muscle groups. The first is the rotator cuff, a group of four tendons and muscles that surround the joint. The rotator cuff is responsible for fine-tuning movement, rotating the arm, and, most importantly, keeping the humeral head centered in the glenoid socket. The second is the deltoid muscle, the large, powerful muscle that covers the shoulder and is primarily responsible for lifting the arm away from the body.
When the Shoulder’s Balance is Lost
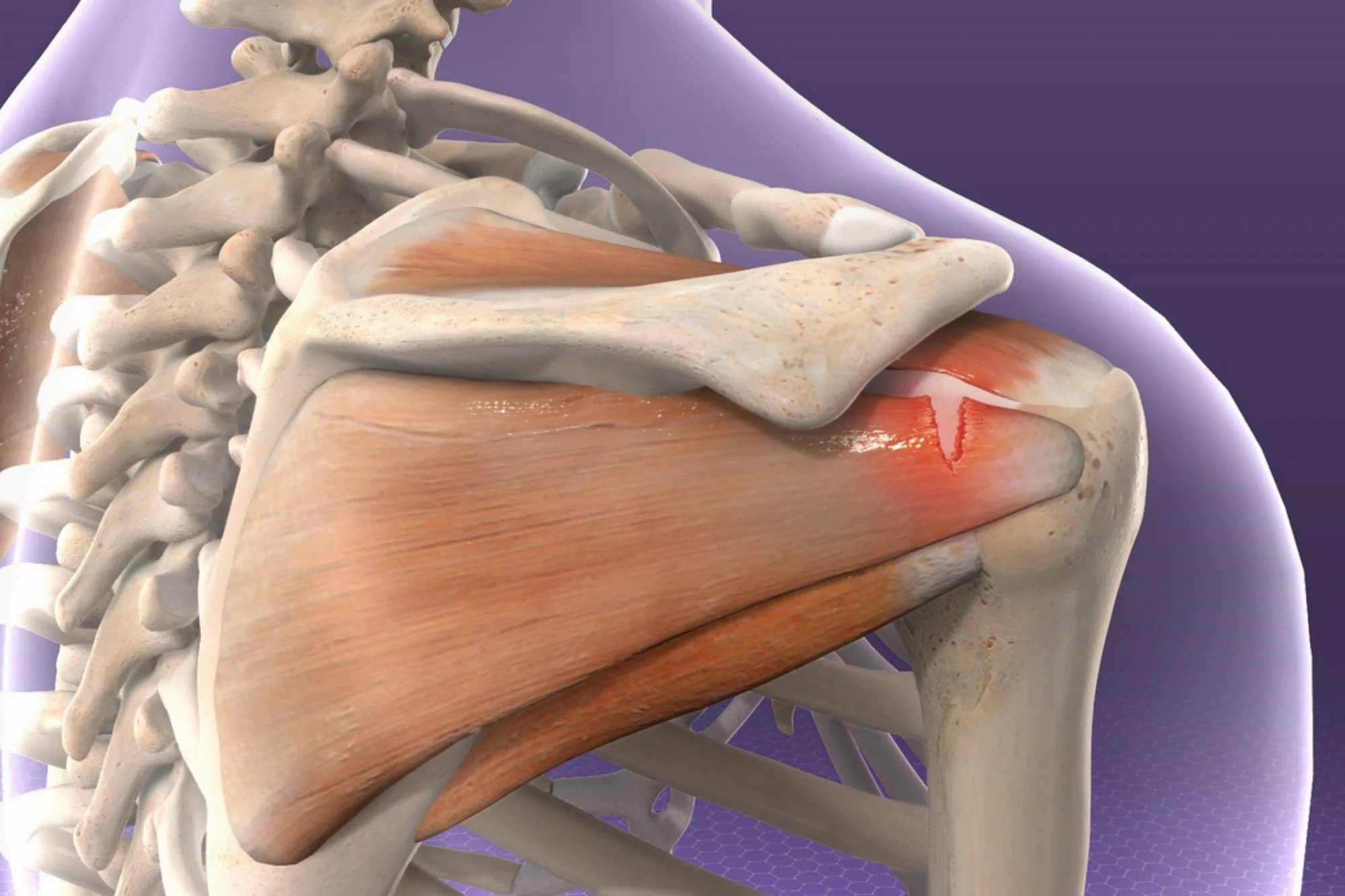
The need for a specialized procedure like reverse shoulder replacement surgery often arises when this delicate balance is disrupted. For example, in cuff tear arthropathy, a massive, long-standing tear in the rotator cuff is present. Without the stabilizing force of the rotator cuff, the humeral head is no longer held in its proper position. It begins to migrate upward, rubbing against the underside of the acromion (part of the shoulder blade). This abnormal friction and instability can lead to arthritis.
A conventional shoulder replacement relies on a healthy, functioning rotator cuff to power and control the new joint. When the rotator cuff is gone, a traditional total shoulder replacement would likely fail to restore function. This is precisely why the reverse design was developed.
What is Reverse Shoulder Replacement Surgery?
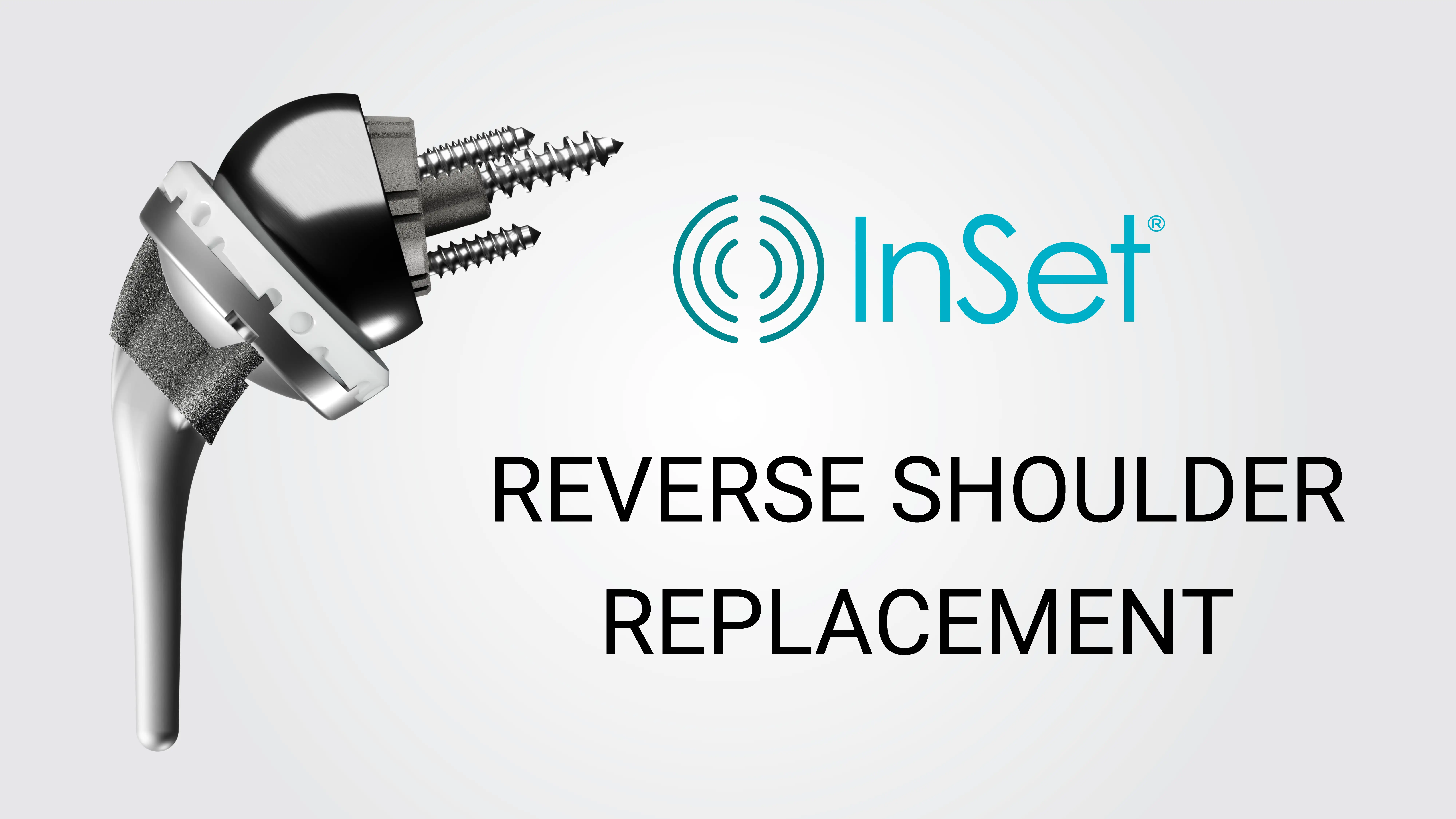
Reverse shoulder replacement surgery is a procedure where the natural anatomy of the shoulder joint is intentionally reversed. In this procedure:
- The Ball is Placed on the Socket Side: A metal hemisphere, or “ball” component (called a glenosphere), is securely attached to the glenoid (the socket side of the shoulder blade).
- The Socket is Placed on the Ball Side: A plastic “socket” component (called a humeral cup) is fixed to the top of the humerus (the upper arm bone).
This new, reversed configuration changes the biomechanics of the shoulder. By moving the center of rotation of the joint, the surgeon is able to place the deltoid muscle under greater tension. This increased tension allows the deltoid muscle to become the primary motor for lifting the arm, effectively bypassing the need for a functional rotator cuff.
Primary Indications: When is This Surgery Recommended?
The decision to proceed with reverse shoulder replacement surgery is a careful one, made in collaboration with an experienced orthopedic surgeon after a thorough evaluation of your condition, medical history, and functional goals. This procedure is generally reserved for specific, complex conditions where a standard replacement would be ineffective or contraindicated.
Cuff Tear Arthropathy
This is a combination of severe, chronic arthritis and a massive, non-repairable tear of the rotator cuff. Patients with this condition often experience severe pain, weakness, and an inability to lift their arm away from their side, a condition sometimes referred to as “pseudo-paralysis.”
Complex Shoulder Fractures
In certain severe, multi-fragmented fractures of the upper humerus, particularly in older patients with poor bone quality, the pieces of the bone may be too small or too numerous to be successfully put back together. In these cases, a reverse shoulder replacement can be used as a primary treatment.
Chronic, Irreparable Rotator Cuff Tears
Even without severe arthritis, a massive rotator cuff tear that cannot be repaired by any other means can lead to significant pain and functional loss. If conservative treatments like physical therapy and injections have failed, a reverse shoulder replacement may be considered.
The Surgical Procedure: A Step-by-Step Overview
Pre-Operative Planning
Before the day of surgery, your surgeon may use advanced imaging, such as X-rays and CT scans, to create a detailed, three-dimensional map of your shoulder anatomy. This allows for precise planning of the implant size and placement. You may also undergo a comprehensive medical evaluation to ensure you are in the best possible health for the procedure.
Anesthesia
The surgery is typically performed under general anesthesia, meaning you will be asleep throughout the procedure. Your surgical team may also use a regional nerve block. This provides pain control immediately after the surgery and can help improve your comfort during the first day or two of recovery.
The Incision
The surgeon makes an incision, typically on the front or top of the shoulder. The exact location and length of the incision may vary based on the surgeon’s preference and the specific needs of your anatomy.
Preparing the Joint and Inserting the Components
The surgeon carefully navigates through the muscles and tissues to access the shoulder joint. The damaged humeral head (the ball) is removed. The glenoid (the socket) is then prepared by removing any remaining cartilage and shaping the bone to accept the new components.
When ready, a metal baseplate is secured to the glenoid bone using screws. The metal hemisphere, or glenosphere, is then attached to this baseplate. This component is now the “ball” of the new joint. A stem is inserted down the center of the humerus (upper arm bone). A plastic liner, which acts as the “socket,” is then attached to the top of this stem.
Final Steps
The new ball and socket are brought together, creating the reversed joint. The surgeon checks the stability and range of motion of the new joint. Once satisfied, the incision is closed with sutures or staples, and a sterile dressing is applied. You will then be moved to a recovery area.
Recovery and Rehabilitation: Your Commitment to Success
The surgical procedure is only the first part of your recovery. While specific timelines and steps may vary, the rehabilitation process is structured and progressive, designed to protect the healing tissues while gradually restoring strength and mobility.
Immediate Post-Operative Period
- Immobilization: You will typically wear a sling to protect the shoulder and allow the soft tissues to heal. It is important to follow your surgeon’s instructions regarding when and how to remove the sling.
- Early Motion: Physical therapy begins almost immediately, but it may be passive motiononly. This means the therapist or another person moves your arm for you. You will be instructed to avoid actively lifting or rotating your arm.
Intermediate Phase
- Active-Assisted Range of Motion: As healing progresses, you may transition to active-assisted exercises, where you use your other arm or a pulley system to help move the operated arm.
- Active Range of Motion: Once your surgeon gives approval, you may begin active range of motion exercises, where you start using your deltoid muscle to lift the arm on your own.
Advanced Strengthening Phase
- Strengthening: This phase may introduce resistance exercises to build strength in the deltoid and surrounding muscles. This is where the functional gains truly accelerate.
- Return to Activity: You may be cleared to return to light work and driving. Your physical therapist will guide you on returning to recreational activities, such as swimming or golf, with modifications.
- Long-Term Improvement: While significant improvement is often seen within the first six months, the strength and function of the shoulder can continue to improve for up to a year or longer after the surgery.
Summary
Reverse shoulder replacement surgery represents an advancement in orthopedic care, offering a possible solution for patients with complex shoulder problems, particularly those involving a non-functional rotator cuff. By reversing the joint’s anatomy, the procedure harnesses the power of the deltoid muscle to restore stability and the ability to lift the arm. The decision to undergo this surgery is a partnership between you and your orthopedic specialist, and a full understanding of what is reverse shoulder replacement surgery, its indications, the procedure, and the commitment required for rehabilitation can help empower you to make the most informed choice for your health and future well-being.
Frequently Asked Questions
How long will I need to wear a sling?
In many cases, patients wear a sling for protection for approximately three to six weeks after the operation. The exact duration depends on the implant and the quality of the soft tissue repair performed during the surgery. Your surgeon will provide specific instructions tailored to your recovery.
Can I return to playing sports?
Many patients return to low-impact activities and sports, such as golf, swimming, and cycling, once they have been cleared by their surgeon and physical therapist. High-impact or contact sports, such as football, rugby, or activities involving heavy, repetitive overhead lifting, are usually discouraged to protect the longevity of the implant.
What is the difference between a reverse and a total shoulder replacement?
The main difference lies in the anatomy and the patient indication. A total shoulder replacement (conventional) maintains the natural anatomy (ball on the arm, socket on the shoulder blade) and requires a healthy rotator cuff. Reverse shoulder replacement surgery reverses the anatomy (ball on the shoulder blade, socket on the arm) and is generally designed for patients who have a non-functional rotator cuff.