The shoulder joint allows for an incredible range of motion. This mobility, however, makes it susceptible to conditions like arthritis, a common source of chronic pain and disability. Patients with arthritis often experience a deep, aching pain that worsens over time, making simple daily activities difficult. A question we frequently hear is, “What causes arthritis in the shoulder?” In this post, we’ll explore the various origins of shoulder arthritis, detailing the different types, the underlying mechanisms of joint damage, and the factors that may increase your risk.
Key Takeaways
- Shoulder arthritis typically falls into five main categories: Osteoarthritis, Rheumatoid Arthritis, Posttraumatic Arthritis, Rotator Cuff Tear Arthropathy, and Avascular Necrosis.
- Osteoarthritis, a common form, results from the progressive breakdown of the joint’s protective cartilage, often due to age and mechanical stress.
- Age, genetics, previous trauma, and repetitive overhead activities can influence the likelihood of developing shoulder arthritis.
The Foundation: A Look at Shoulder Anatomy
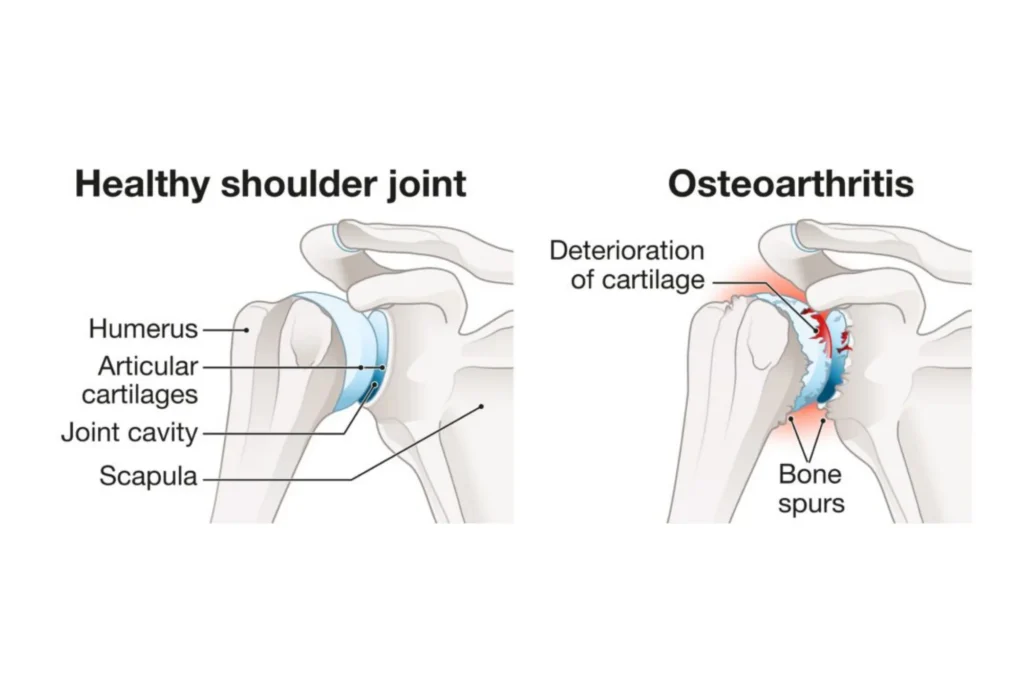
To truly understand what causes arthritis in the shoulder, we must first appreciate the joint’s structure. The shoulder is a complex of several joints, muscles, and tendons. The primary joint affected by arthritis is the glenohumeral joint, the main ball-and-socket joint where the humerus (ball) meets the glenoid (socket). Articular cartilage covers these surfaces, acting as a cushion to allow effortless gliding. Synovial fluid lubricates and nourishes this cartilage.
When arthritis develops, this system breaks down. The cartilage can wear away and the bones may begin to rub together. The resulting friction causes inflammation, pain, and stiffness. The acromioclavicular (AC) joint, which connects the collarbone to the shoulder blade, is the other joint commonly affected.

The Five Primary Causes of Shoulder Arthritis
Shoulder arthritis is not a single disease. It is an umbrella term covering several conditions that lead to joint inflammation and cartilage loss. Each type has a distinct origin and progression.
1. Osteoarthritis (OA)
Osteoarthritis, also called “wear-and-tear” arthritis, is a progressive degenerative joint disease. It commonly affects people over the age of 50. The underlying cause is the gradual breakdown of the articular cartilage.
The cartilage loses elasticity, becoming frayed and rough. This process narrows the space between the bones and may eventually lead to “bone-on-bone” arthritis. This friction generates pain and limits motion. The body may attempt to compensate by forming small bony growths called osteophytes, or bone spurs, which can further restrict movement.
While the exact cause of osteoarthritis depends on the patient, it frequently involves a combination of mechanical stress, genetic predisposition, and biological processes. For many, it appears to be a consequence of aging and lifelong use, where the cumulative effect of decades of shoulder use overwhelms the cartilage’s ability to repair itself.
2. Posttraumatic Arthritis
Posttraumatic arthritis develops after a physical injury to the shoulder joint. The injury itself triggers a cascade of events that ultimately leads to cartilage destruction. This type of arthritis can affect people of any age.
A significant trauma, such as a fracture of the humerus or glenoid, or a shoulder dislocation, can disrupt the joint’s smooth mechanics. Even after successful surgical repair, the initial damage to the cartilage may be irreversible. The joint surfaces may no longer align perfectly, creating abnormal pressure points that experience excessive friction and wear. This accelerated wear and tear causes the cartilage to break down much faster than normal.
The onset of symptoms is frequently delayed. Patients may feel fine for years after the initial injury, with pain and stiffness only beginning to manifest five, ten, or even twenty years later. This delay can obscure the connection to the old injury, making a thorough medical history essential for accurate diagnosis.
3. Rheumatoid Arthritis (RA)
Rheumatoid arthritis is an autoimmune disease. This means the body’s immune system mistakenly attacks its own healthy tissues. In the shoulder, the immune system targets the synovium, the lining of the joint capsule.
This attack causes the synovium to become inflamed and swollen, a condition called synovitis. This inflammation is destructive, producing chemicals that erode the articular cartilage, underlying bone, and surrounding soft tissues like ligaments and tendons. RA typically affects multiple joints throughout the body and is commonly symmetrical, meaning it can affect both shoulders at the same time. As a systemic disease, RA may require a different approach to treatment than mechanical wear.
4. Rotator Cuff Tear Arthropathy
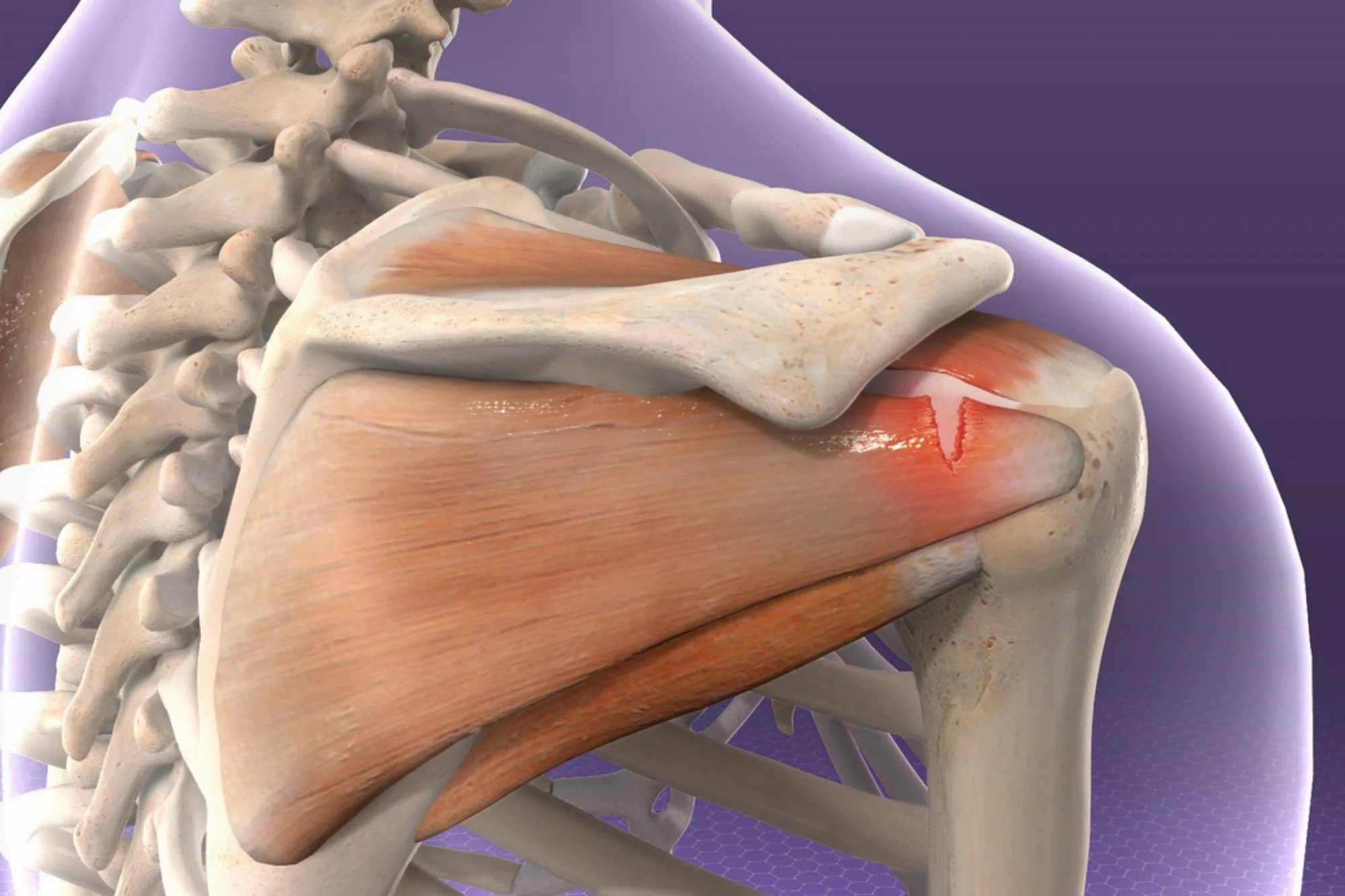
This form of arthritis develops in the presence of a massive, long-standing tear of the rotator cuff tendons. The rotator cuff muscles normally provide stability, holding the head of the humerus in the glenoid socket. When a large tear occurs, this stabilizing function can be lost.
The humeral head begins to migrate upward, moving out of its normal position. It then rubs against the acromion, the bony roof of the shoulder. This abnormal contact and friction can rapidly destroy the articular cartilage. The combination of a non-functional rotator cuff and advanced arthritis is known as rotator cuff tear arthropathy.
Patients with this condition experience severe pain and significant weakness, often unable to lift their arm away from their side. This condition may require specialized surgical techniques, such as a reverse total shoulder replacement.
5. Avascular Necrosis (AVN)
Avascular necrosis, or osteonecrosis, is a less common cause of shoulder arthritis. It involves the death of bone tissue in the humeral head. This occurs because the blood supply to that area is disrupted. Bone cells need a constant supply of blood to survive.
The dead bone gradually weakens and collapses, which damages the smooth articular cartilage covering the bone. As the joint surface becomes irregular, it leads to the rapid development of arthritis. The glenoid socket can also be damaged as the collapsed humeral head grinds against it.
Several factors may interrupt the blood flow to the humeral head. Possible risk factors include high-dose or long-term use of corticosteroid medications, heavy alcohol use, certain medical conditions, and trauma. Sometimes, no clear cause is identified, which doctors refer to as idiopathic AVN.
Factors That Increase the Risk of Shoulder Arthritis
While the five types of arthritis describe the mechanism of joint destruction, several risk factors may make an individual more susceptible to developing the condition. Understanding these factors can help patients and doctors take proactive steps.
Age and Genetics
Age is a risk factor for osteoarthritis, as the wear-and-tear process accumulates over decades. Most cases of glenohumeral osteoarthritis occur in individuals over the age of 50, though age is less of a factor in posttraumatic arthritis or RA.
Genetics also plays a role. If close family members have experienced severe arthritis, you may have a higher predisposition due to genetic markers that influence cartilage quality and inflammatory response.
Previous Injury or Trauma
As discussed with posttraumatic arthritis, a history of shoulder injury increases risk. This includes fractures of the humerus or glenoid, recurrent shoulder dislocations, and even seemingly minor injuries that alter the joint’s biomechanics. Previous surgery, even when necessary, can also be a risk factor if it changes the joint’s alignment or stability, potentially contributing to later arthritic changes.
Repetitive Stress and Occupation
Repetitive overhead activities place stress on the shoulder joint. Athletes (e.g., baseball pitchers, swimmers) and certain occupations (e.g., construction workers, painters) often face an elevated risk. This chronic microtrauma can accelerate the breakdown of articular cartilage, potentially contributing to the development of osteoarthritis or rotator cuff tears that lead to arthropathy.
Systemic Health Conditions
Several systemic conditions can contribute to the development of shoulder arthritis. Rheumatoid arthritis is the most obvious example, but other inflammatory conditions and metabolic diseases may also play a role. Maintaining overall health and controlling chronic inflammation may help protect the joints.
The Progression of Shoulder Arthritis
Arthritis is typically a progressive condition, starting subtly and worsening over time. Recognizing the early signs is important for timely intervention.
Early Stages
In the early stages, pain may be intermittent, occurring only with specific activities, or a mild ache after a long day. Stiffness may be minimal, noticeable only in the morning or after rest. At this point, the cartilage is only beginning to fray, and the joint space is relatively preserved.
Advanced Stages
As the condition progresses, symptoms may become more constant. Pain can be present even at rest, and night pain often disrupts sleep. Stiffness becomes severe, and patients lose a significant amount of their range of motion, struggling to reach behind their back or overhead. The grinding sensation, or crepitus, can become more pronounced.
Diagnosis: Pinpointing the Cause
The diagnostic process typically involves a thorough medical history and a physical examination, where your doctor assesses the nature of the pain, its location, onset, and the range of motion and strength of the shoulder.
Imaging studies can help support the diagnosis. X-rays are the primary tool, showing the extent of joint space narrowing, the presence of bone spurs, and any upward migration of the humeral head that suggests rotator cuff tear arthropathy. In some cases, an MRI may be necessary to better visualize soft tissues like the rotator cuff tendons and the cartilage itself. Blood tests may be ordered if an inflammatory type of arthritis, such as rheumatoid arthritis, is suspected. A CT may also be ordered, especially for surgery planning.
Treatment Options
Conservative treatments form the cornerstone of early management, aiming to reduce pain, inflammation, and maintain joint mobility.
- Physical Therapy: Specific exercises strengthen surrounding muscles, improving stability and function, and teaching techniques to protect the joint.
- Medication: Nonsteroidal anti-inflammatory drugs (NSAIDs) may help control pain and inflammation.
- Injections: Corticosteroid injections provide strong yet temporary relief, and newer options like platelet-rich plasma (PRP) are also being explored.
When conservative measures fail, surgical options become a consideration, ranging from arthroscopic procedures to shoulder replacement. The choice of surgery depends entirely on the specific cause and severity of the arthritis. For example, a reverse total shoulder replacement is often the recommended option for rotator cuff tear arthropathy, while a standard total shoulder replacement is typically used for severe osteoarthritis with an intact rotator cuff. An experienced shoulder specialist can evaluate your condition and help guide the most effective treatment path.
Summary
Shoulder arthritis doesn’t have a single cause. It can result from years of natural joint wear, an autoimmune condition, a previous injury, or even long-standing tendon damage that alters how the shoulder moves. Conditions such as osteoarthritis, post-traumatic arthritis, rheumatoid arthritis, rotator cuff tear arthropathy, and avascular necrosis all can damage the smooth cartilage that allows the shoulder to move comfortably. As this cartilage breaks down, pain, stiffness, and loss of function often follow. Today’s orthopedic treatments offer various ways to help manage pain, restore movement, and improve quality of life. If shoulder pain is holding you back, a professional evaluation may help uncover the cause and guide you toward the right path forward.
Frequently Asked Questions (FAQ)
Does every shoulder injury lead to posttraumatic arthritis?
No, not every shoulder injury will lead to posttraumatic arthritis. The risk, however, is higher with severe injuries. These may include complex fractures involving the joint surface or recurrent, unstable dislocations. The key factor is the degree of initial damage to the articular cartilage and the resulting change in joint mechanics.
Can I prevent shoulder arthritis?
You may not be able to prevent all forms of shoulder arthritis, especially those linked to genetics or autoimmune disease. However, you can take steps to help reduce your risk of some types. Avoiding repetitive, heavy overhead lifting when possible can be helpful. Prompt and proper treatment of any shoulder injury, such as a fracture or rotator cuff tear, is also essential. Regular, gentle exercise to maintain shoulder strength and flexibility is highly recommended.
What is the difference between glenohumeral and AC joint arthritis?
The difference lies in the location. Glenohumeral arthritis affects the main ball-and-socket joint, where the humerus meets the glenoid. The pain is typically felt deep in the shoulder or in the back of the shoulder. AC joint arthritis affects the joint at the top of the shoulder. This is where the collarbone meets the acromion. The pain from AC joint arthritis is usually localized directly on top of the shoulder.